
Hey guys, Dr. Lell here explaining another common condition in an easy to understand way. Last week, I blogged about disc herniations and today I want to explain something very closely related and in times, a precursor. I’m talking about the bulging disc. My patients recognize this as a “squishy disc”…you won’t find that term in any textbook.
Think of bulging discs as a ticking time bomb that may never go off and having one doesn’t always mean you’ll feel pain. It’s an often overlooked but very common cause of “nonspecific” low back pain. Unlike the herniated or blown disc, the bulging disc isn’t necessarily caused by any one event. It spans all ages (though it’s less common in older people) and activity levels.
What is it?
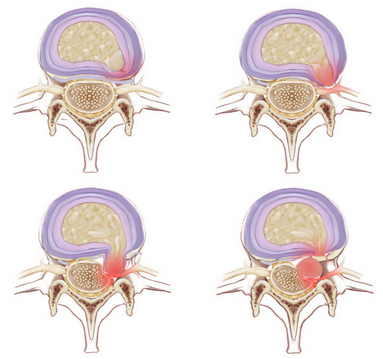
Take a look at the picture below. For a more detailed review of the anatomy, please read this. To review, the disc is a jelly-like center wrapped by a thick outer covering. As pressure in the disc increases (while sitting, straining, lifting, etc.) the jelly presses up and pushes against the outer covering (top left picture). If that outer covering is weak (from repetitive strain, smoking, or moving improperly just to name a few) it can give a little and start to protrude (top right). This alone can be painful and can cause pain in the low back that may radiate into the butt. It may cause the muscles in the low back, butt, and hamstrings to lock up as a protective mechanism and may put slight pressure on a nerve. The bottom pictures are representative of a disc herniation, which the bulge could turn into.
How do I know if I have this?
Symptoms may include the following…
- It may or may not be painful. It’s typically low back tightness with or without pain into the butt.
- The “pain” is worse in the morning or with getting in/out of a car or bed or up from a chair
- Chronically tight hamstrings
- Inability to touch your toes
- A leg that doesn’t seem to be as strong or “able” as the other
How is it treated?
This is largely a functional condition. The best treatment, especially if it isn’t painful, is education about how to move your body and exercises that can be done at home to strengthen the area and prevent further “squishiness” or a potential herniation. The way that you move, lift, and bend is what caused this and it can be the way that you fix it. The degree of treatment really relies on the degree of severity and the other associated risk factors. For example, someone that handles luggage for an airline may need more rehab exercises than someone who walks dogs. Someone with occasional back tightness will need less than someone with an occasionally numb foot. I typically start by reducing the pain and symptoms (if there are any) and then setting up a great home based program for people to maintain and work on preventing future episodes.